NHS Culture Blog
|
10 October 2019
I’m a Waspi. A 1950’s woman who has been told that I have lost about £40.000 through two alterations to my state pension age. I have never received a letter from the DWP notifying me of these changes. Discourteous and sloppy at the very least. Unjust and unfair regarding process, penalising one group of women disproportionately, at worst. Recently the organisation Back to 60 lost their judicial review challenging the changes and the way the process has been conducted. The outcome is extremely disappointing for about 3.8 million women across the UK. I was particularly interested in one of the arguments of the government. The QC Sir James Eadie stated that the ‘Parliament has no substantive free standing obligation to fairness’. Sadly, the judges appear to have agreed with this statement. I found it quite shocking. Logic indicates that if there is no obligation to fairness and justice, then there is a right to be unjust and unfair. There is therefore no moral accountability at the heart of our Parliament and administration. Perhaps this goes to the core of some of our problems in this country? Perhaps it helps to explain the appalling responses to various scandals e.g. Hillsborough, Mid Staffordshire, Morecambe Bay, Gosport, Southern Health, deaths of children in Northern Ireland and the shameful failures regarding the contaminated blood. People fighting for years to get answers, and some fairness and justice. Governments displaying differing degrees of ‘deafness’. It seems almost impossible for people to get justice and redress for parliamentary and institutional failings. A shocking failure to deliver timely accountability. Delivering fairness and justice is not our natural default in the UK. Withholding and trying to block it seems to be. That needs to change. ‘When justice rules a nation, everyone is glad; When injustice rules, everyone groans.’ Proverbs 29 v.2 The Poverty and Justice Bible
0 Comments
26 August 2019
‘Whistling in the wind’ is a very dangerous activity in the NHS. This is clearly shown in the recent book ‘Whistle in the Wind’ by Dr Peter Duffy, a consultant surgeon in urology. ‘It is difficult to describe the sheer intensity of the hatred that can characterise high profile NHS whistle-blower cases. Numerous lives and families have been destroyed by the ferocious retaliation that has followed expressions of concern within the NHS and the breaking of the unwritten code of National Health Service ‘omerta’ (p.229). He clearly identifies behaviours that are in the APPG ‘Cycle of abuse’ (see July and August blog posts), and some of the negative behaviours described in the report ‘How doctors in senior leadership roles establish and maintain a positive patient-centred culture: Research Report for the General Medical Council’ by Dr Suzanne Shale. The book very sadly details the depressing, and all too familiar, responses to raising concerns and ‘truth telling’ in the NHS. The intimidation and victimisation of the ‘truth teller’, with the resulting stress, illness and damage to career. The non-response to concerns. Underpinning this is the relentless pressure and chaos within the system and the toleration of excessive, unreasonable workloads and bad practice. Poor and mediocre treatment of the patient seems to be acceptable. There is obviously an organisational lack of concern for the welfare of patients. Rather than quality and safety being the priority, other factors dominate, such as the need to achieve targets and protection of self-interest. Allegations of racism also appear to be of greater priority than ensuring patient safety; clearly a perverse and distorted priority. Some people who failed to deliver high quality care apparently protected. The manipulation of waiting lists, for reasons of self–interest via well remunerated extra clinics, was described. Patients were also off-loaded onto other consultants to avoid taking responsibility and action. Are these practices common across the NHS? Peter Duffy considers there is a ‘…longstanding, toxic and dishonest culture’ in the NHS (p.231). He also describes the culture that existed at Morecambe Bay, only months after the publication of the very damming Kirkup report about the trusts maternity services. ‘Once again, it appeared that Morecambe Bay had tolerated a string of errors, with patients’ lives being risked, direct harm to patients, episodes of neglect and an overwhelming culture of lassitude, cover-up, deceit, bullying and complacency. Cover up and carry-on was back as the organisational norm.’ (p.113). He believes that ‘…there needs to be a comprehensive change within senior management and senior members of the medical and nursing professions in the NHS. All too often, senior clinicians, managers and executives are bent upon self-promotion, advancing their own careers ahead of others by giving the impression of being a ‘safe’ pair of hands, suppressing dissent and ruthlessly dealing with anything that might represent a threat or poor publicity for themselves, the greater organisation or ‘the Minister’…anyone stepping out of line can expect no mercy’ (p.231). There is systemic dysfunction, many avoidable deaths and damage to patients in the NHS. The central focus has to be upon the well-being and safety of patients. The NHS needs a very hefty dose of honesty and integrity; a major ‘clean up’ in the way that it conducts business. 16 August 2019
Returning to the APPG report for Whistleblowing. ‘Whistleblowing: The Personal Cost of Doing the Right Thing and the Cost to Society of Ignoring it’ https://docs.wixstatic.com/ugd/88d04c_9754e54bc641443db902cd963687cb55.pdf I have observed that in reports there is often little mention of HR as a function and their role in enacting bad practice in organisations. It is as if HR are not there. This report makes reference to HR three times. 1) ‘One respondent reported that, after refusing to provide evidence of investigations into the grievance raised, the HR officer behaved in ‘an extremely confrontational and unprofessional manner’. In the ensuing meeting, described as ‘difficult and threatening’, the whistleblower was made feel as if [she/he] was ‘a liar and a troublemaker’. Another respondent reported that [they] were called to a disciplinary meeting, threatened with dismissal for a minor mistake. Another one wrote that she/he was criticised and ‘warned […] as to future conduct.’ (p.24) 2) ‘Sometimes the dismissal follows disciplinary action. One respondent wrote that after having blown the whistle, the HR office advised her/him to file a grievance, but when she/he did so, the organisation (a hospital charity) immediately ‘threatened [her/him] with the sack’. They then carried out an investigation against her/him and she/he was eventually dismissed, despite the HR consultant had supported her/his case.’ (p.26). 3) ‘The [NHS] FtSU scheme attracted significant criticism for failing to protect or support whistleblowers. The lack of confidence in the system was corroborated by a whistleblower who had left after being targeted for supporting a whistleblower. Further comments alleged that the guardians were using the role as a career stepping stone and that many of the guardian posts had been filled by HR with too few medical staff.’ (p.30). There are, however, ten references to ‘disciplinary action’, e.g. ‘While some accusations against whistleblowers remain merely informal, some are turned into disciplinary action against whistleblowers. Sometimes, disciplinary proceedings are used as a means to perpetrate any of the above retaliatory conducts, such as ostracising or intimidating whistleblowers, to the purpose – as reported by one respondent – to ‘cover up management failings’.’p.25). Other words are also used such as demotion, suspension, dismissal, and formal action. All of which are administered by HR personnel. The HR function is at the core of the APPG ‘Cycle of abuse’. They might at times be enablers of good practice, but they can also be enablers of very bad and damaging practice. There to protect the organisation and the managers, and sadly, as quoted above, to ‘cover up management failings’. There seems to be a lack of ethics and morality in the way they conduct their role. One of my NHS research participants said the following: “I think it’s sad that when you get a genuine whistle-blower raising concerns about standards of care. That somehow HR always seem to be on the opposite side of the line to that individual or individuals. And supporting a hard line management approach rather than again, as I would say, looking at it in terms of what is this service supposed to be about? It’s supposed to be about providing, you know, the best possible safest care for patients.” Other NHS participants saw HR as a ‘management tool’. “...101% in league with managers, and biased as hell”, as “...organisations hatchet men”. HR personnel were viewed as people who are distant, detached and separate from staff. Not seen as effective and not instructing the “...proper way of doing things”. Perceived as being aware of problems, but not taking action. People question whether many HR departments know what bullying is, or have any idea how to investigate it. They encourage, and “...facilitate bullying on many occasions”. There can be “...bullying at the top level, but HR is in the middle of it”. One person thought HR were corrupted and “...embroiled in organisational failure”. “HR directors they’re...they’re corporate, and...they’re ‘singing a corporate tune’, and...detached as those bad detached NHS managers of all sorts really”. There is an urgent need to review the role of HR in whistleblowing cases. 28 July 2019
In July of this year the All Party Parliamentary Group (APPG) for Whistleblowing published the first of its three reports - ‘Whistleblowing: The Personal Cost of Doing the Right Thing and the Cost to Society of Ignoring it’ https://docs.wixstatic.com/ugd/88d04c_9754e54bc641443db902cd963687cb55.pdf The focus of this report is upon the experiences and opinions of whistleblowers themselves. The work covers all work sectors, but gives three examples from across the NHS, that of Gosport, Mid-Staffs, and Morecombe Bay hospitals, where the message of the ‘truth tellers’ and whistleblowers was rejected. The Forward states that ‘On 10th July 2018 we held our inaugural meeting, well attended by MP’s, whistleblower constituents, the press and civil society organisations. Gosport Memorial Hospital was in the news that day, how whistleblowers had been ignored or silenced and how if they had been heeded lives could have been saved.’ Stephen Kerr MP (Chair of the APPG) goes on to say that ‘Whistleblowers are the first line of defence against crime, corruption and cover ups’ and ‘This report shines a light on a culture that too often supports the covering up of wrongdoing and the penalising of whistleblowers. With increasing focus on organisational culture and new global laws and regulations to support transparency and whistleblowers, the UK needs a comprehensive, transparent and accessible framework and an organisation that will support whistleblowers and whistleblowing.’. The report covers in some depth the ‘Cycle of abuse’. None of this will be of surprise to anyone who has watched the behaviour of NHS organisations when responding to ‘bad news’ and a challenge to authority. They don’t like ‘dirty linen’ being ‘washed in public’, and having their ‘shiny image’ tarnished. Following reporting of a concern there is some, or all, of the ‘Cycle of abuse’:
A multiple of recommendations are made by the APPG including the banning of NDAs. We can only hope that this report has an impact, and that parliament finally wakes up to the importance of supporting and protecting ‘truth tellers’/whistleblowers in all the different sectors. It will benefit us all. 15 June 2019
I have recently read ‘Denial: The unspeakable truth’. A difficult and uncomfortable read. I was made aware of this book through the Radio 4 programme ‘The age of denial’ (https://www.bbc.co.uk/programmes/m000357l/episodes/player). The author Keith Kahn-Harris considers denial and denialism. Denial and denialism are closely linked, and denialism is “…dangerous” (p.4) and “…deeply poisonous” (p.ix). Denialism is defined as an “…expansion, an intensification, of denial. At root, denial and denialism are simply a sub-set of the many ways humans have developed to use language to deceive others and themselves. Denial can be as simple as refusing to accept that someone else is speaking truthfully. Denial can be unfathomable as the multiple ways we avoid acknowledging our weaknesses and secret desires. Denialism is more than just another manifestation of humdrum deceptions and self-deceptions. It represents the transformation of the everyday practice of denial into a new way of seeing the world and – most importantly to this book – a collective accomplishment. Denial is furtive and routine; denialism is combative and extraordinary. Denial hides from the truth; denialism builds a new and better truth.” (p.2-3) Does the NHS, and structures around and external to the Fortress NHS exhibit denialism? The NHS certainly exhibits denial. An NHS whistleblower in a blog (Alexander, 2016) described the regulator, the Care Quality Commission, as being part of “…the NHS denial machine”. A research participant, a cognitive behavioural therapist, wrote that the NHS culture was “Complicated; Unhelpfully competitive; Delusional. Though this seems to be negate those who do a lot of good work despite it all, so if I was to add a fourth, it would be ‘Heroic’. [Delusional?] Elephant in the room stuff. The culture is deluded and deluding by pretending the [Negative] behaviours described…don’t exist. Like a family that has a terrible secret that is not discussed and has a shared delusion that everything is OK” There is a fierce resistance to any ‘bad news’ and negativity, and a great desire for ‘good news’. A risk manager referred to the “…good news factory”. “It is very tempting to join the club and be part of the ‘good news factory’. I dip in and out of that. Trying to protect the organisation, but also trying to protect the interests of patients and staff as an advocate…They [Directors] don’t care about anything else as long as not reported.” R “Talk a bit more about the ‘Good news factory’. Is that a term you use normally?” “Not used it before. It’s like, no... Somebody told me, ‘Iced cake syndrome’. Lovely on the outside, mouldy on the inside. Part of a culture being led by the government. Present a pretty picture fed up to the voters. Underneath it’s a bit of a shambles.” An HR manager said “It’s a ‘stopping bad news factory’…rather than ‘good news’”. “There are many cultures within NHS organisations, but a common denominator with each is defensiveness”. Certainly the denial is a collective accomplishment within the NHS and the structures around it. It is most definitely combative. This is particularly seen when organisations come up against whistleblowers or ‘truth tellers’, the term Graham Pink prefers (A time to speak: Diary of an NHS whistleblower, 2013). ‘Truth tellers’ are ruthlessly pursued and systematically attacked for raising concerns about ill-treatment of both patients and staff. Careers are destroyed. Many NHS staff, particularly senior managers, will go to great lengths to avoid facing reality. The NHS constantly presents a “…new way of seeing the world” and “…builds a new and better truth” with attempts to redefine reality. There is The Great Pretence that things are, what they are not. That Pretence is indeed deeply poisonous and dangerous as it prevents any positive change and improvement. 2 June 2019
On the day of the European elections The Telegraph editorial wrote, referring to Mrs May, that ‘Her resistance to facts is absurd’. Sadly, this statement could apply to many politicians in this country, of all persuasions. This same resistance to facts and ‘knowing’ is also constantly seen within NHS services. In that same paper is the headline ‘Autistic NHS patients ‘were tortured by staff’. The Panorama programme about Whorlton Hall (22 May 2019) told us that whistleblowers were ignored and no action was taken to address complaints about the quality of treatment delivered (https://www.bbc.co.uk/iplayer/episode/m00059qb/panorama-undercover-hospital-abuse-scandal). Anyone who watches the Panorama programme has to be appalled at what was done to vulnerable and terrified people. The Patient Experience Library recently shared the link to the ‘Report: Review of Maternity Services at Cwm Taf Health Board.’ These are the conclusions (https://www.patientlibrary.net/tempgen/194266.pdf). ‘Clearly, the review of the process for handling and responding to complaints and concerns and governance is a priority; interviews and engagement with women and families revealed serious issues about the way that concerns and complaints were investigated and responded to. Issues included:
In both situations people were not listened to and there was a failure to respond. There is a very strong resistance to any ‘bad news’ or criticism in the NHS. When there is resistance to facts and ‘knowing’ it is indeed absurd, as improvement then becomes impossible. 14 April 2019
I was particularly interested in the description of the ‘Fortress NHS’ by David Seedhouse as one of the research participants described the NHS as ‘The Citadel’. “It can be a career ending move to, um, raise concerns with NHS managers. Basically another element of the culture is, you ‘keep the lid on’, you ‘don’t expose your dirty linen in public’. And if people want to do that, you attack them professionally, personally, you make them go and see psychiatrists. You, if they beat you at an industrial employment tribunal, you pursue them for costs. There is no end to what the NHS will do to people who try to break open The Citadel.” R - Please could you tell me a little more about The Citadel? “The Citadel is the notional home of the big secret that the NHS cannot do better than killing an awful lot of people and treating tens if [not] thousands, largely elderly, in an appalling manner...The Citadel is a metaphor for the NHS - picking up on AJ Cronin's title. Its primary purpose is to protect itself even though the public believe it is there solely to make them better. When individuals see what's going on in The Citadel and try to advertise it they will generally be repulsed. [They] broke down the walls of The Citadel because among other things it suited a new ruler to help…to break them down. Now many of the insiders are wondering how to respond to being on display; first response, pretend nothing has happened and hope that the walls can be rebuilt” Of course secrets often go together with lies, and there are a number of references to ‘lies’ in the literature. ‘The NHS is likened to East Germany with the Stasi security police, with their use of ‘...euphemisms, double speak and downright lies’ (Riddington Young et al., 2008, p.14). There are ‘big lies’ (Taylor, 2013) and myths, lies and deception (Davis, Lister and Wrigley, 2015). The facts need to be denied and the ‘…political spin machine goes into overdrive’ (p.40). Lies take different forms to justify actions and the ‘…first casualty was truth’ (p.39). There is misrepresentation and concealment.’ (unpublished – Pope, 2019, ‘The NHS: Dysfunctional cultural characteristics’). On 8 April 2019 Andy Cowper in the Health Service Journal wrote ‘Cowper’s Cut: The price of financial lying’ - ‘The NHS will have to pay the price for cultivating a culture of financial lying and cheating and incentivising the wrong things’. What is clear is that ‘The Citadel’ and ‘Fortress NHS’ and the secrets within it are fiercely guarded and protected. People go to great lengths to prevent the exposure of ‘dirty linen’. Secrets are kept unless people are able to break down the walls. ‘The Citadel’ is a dark place. 14 March 2019 I am in the process of reading a very interesting book by David Seedhouse, ‘Fortress NHS: A philosophical review of the National Health Service’. Written in 1994 he thinks the ‘…present proprietors of the NHS show no qualms about implementing tough practical measures to prohibit free speech (p.28), so again nothing has changed. Paper six entitled ‘Fortress NHS’ provides a description of the structure of the Fortress (see diagram below). There are the outer walls which are part of its ‘shield’. ‘The key components of the outer structure of the fortress are mythology (the continuing faith of the British people – most of them outside but some within – that the NHS is fully and coherently principled); the results of political compromise (both at the outset and throughout the development of the health service; hierarchy, internal regulations and discipline (used – increasingly these days with the advent of the manager – to minimise both protest and innovation); and professional and personal self-interest (disciplines and individuals benefit from working for the NHS and so have developed a range of methods to ensure that they continue to do so’ (p.99). There are ‘perimeter strongholds’. These are peopled by those ‘…external to the NHS who have a strong financial interest’ in the NHS such as the drug companies and other manufacturers. ‘The drug industry in particular is a powerful ally, indeed some would say it is part of the Fortress’ (pp.99-100). Other security systems and defences are in place inside the walls, ‘…behind the existing wall of mythology’ (p.101). ‘Fortress NHS has found it necessary to employ tactics which some might choose to describe as brainwashing’. There are four types of defences. 1. Use of special meanings ‘…words which have well known meanings in everyday life are given new and different meanings within the Fortress’ (p.101); a contortion of meaning. E.g. ‘Inside the Fortress quality is cheap’ (p.102) 2. Esoteric use of language Excessive use of technical language 3. Creation of an artificial framework This defence works by ensuring that the ‘…special meanings and use of language seem normal and not contrived’ with the result of a ‘numbing effect on the intellect’ (p.101) 4. Rhetoric is used incessantly Everyone begins to talk in the same way. One of my research focus groups discussed how acronyms prevented thought: M Yes, they come across as feeling threatened, but also they are trying to control the definition of um, what can be talked about, aren’t they? They are sort of, and they are hoping that if nothing gets talked about, nothing can be thought about G And then nothing needs to be done M And then nothing needs to be done, so uh, Orwell talks about in 1984, he talks about how acronyms are used to stop people thinking. The NHS is full of acronyms for example. So the relevance of what I am saying is, so if you talk constantly in terms about GB4’s and… M All these sorts of things people have, this language in talking that closes down, makes it impossible to think A People don’t know what acronyms mean half the time G Yeh, that’s right M They don’t know how to think about. It closes down thinking, so in this way I think, it’s a kind of, also probably not a conscious strategy, but it is a way of trying to close down conversation, thinking, people trying to do, you know, people trying to get engaged with the issues A This is confidential OK. But the e-mail we had recently from our manager contained two or three acronyms and I didn’t understand two of those… A I’ve worked here for twelve years, got no idea what those two acronyms mean. That one I know, those two, have never heard of before. As a consequence I had no, I really didn’t understand G There is a lot of those... A Why I was supposed to know? S It’s like the NHS has always had that hasn’t it?... G Yes, yes… M What it boils down to I think is who defines what can be talked about, what the truth is, how something can be understood. Who’s got the power to do that? And they are using their power in an absolutely obnoxious way 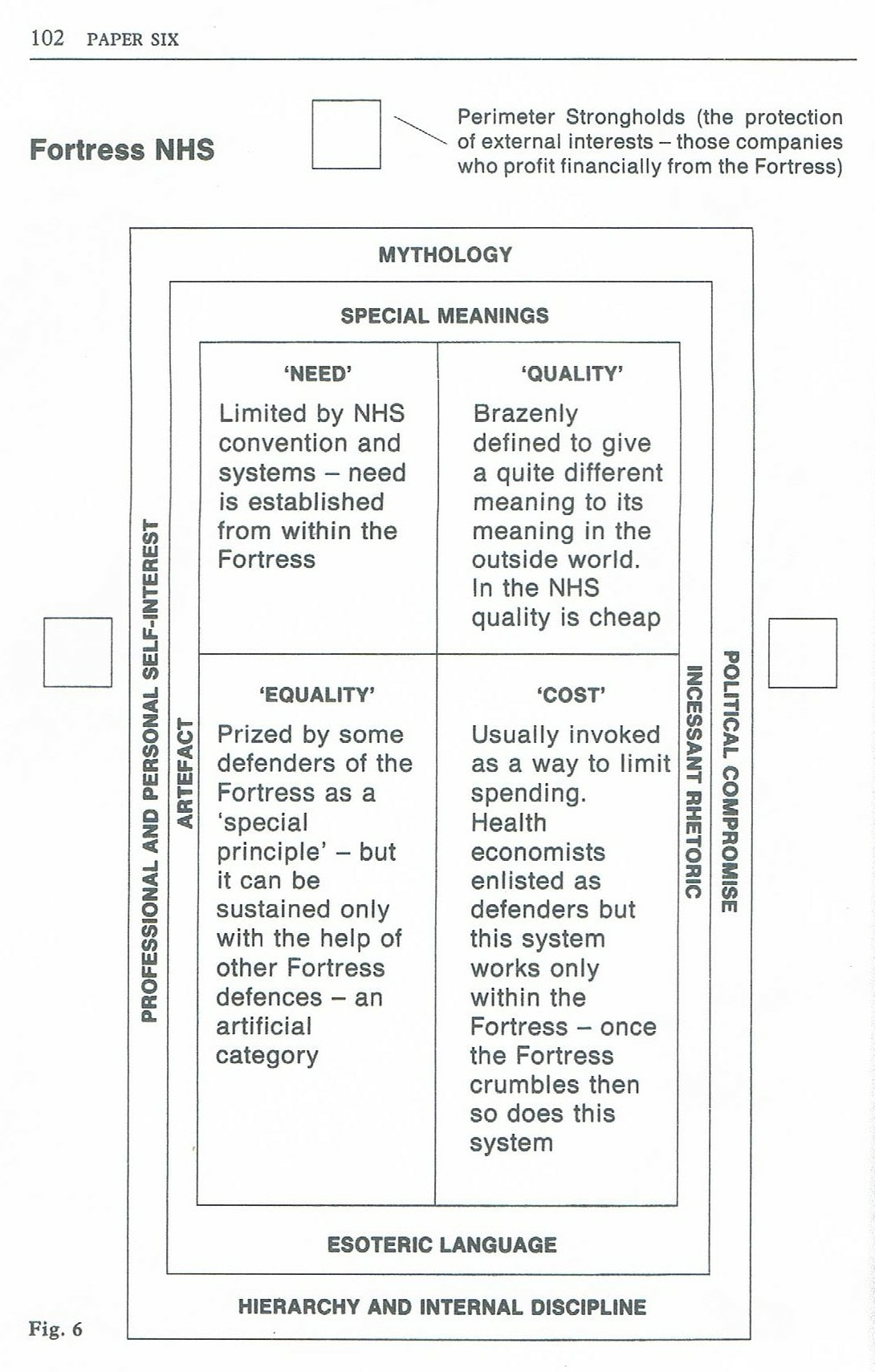 The NHS has ‘pockets’ and ‘islands’ of a positive culture. However, my research concluded that the NHS is institutionally and systemically deaf, bullying, defensive and dishonest (Pope 2017). The dishonesty is seen in a number of ways. It can be the overarching pretence that things are what they are not, and the promotion of ‘good news’ and spin. It can be the blatant lying and ‘cover up’ in the face of failure. Often records and notes ‘disappear’. The NHS is very defensive and is exquisitely sensitive to anything that dents and threatens to tarnish its reputation and image of perfection.
Scandal of infected imported blood products: A news item on the Radio 4 programme (11 Feb 2019, 1.53:45) was about the scandal of the importation of infected Factor 8 in the 1970/80’s. There have been 1500 confirmed deaths. Jason Evans describes the situation as a “cover up that’s been going on for decades”. There was a recent internal government audit which showed that 1000 files relating to the cases were removed by civil servants. The DH has now apparently said that many of these have been found. Morecombe Bay: The KIrkup Morecombe Bay report (2015) identified collusion and concealing of the truth. ‘Many of the reactions of maternity unit staff at this stage were shaped by denial that there was a problem, their rejection of criticism of them that they felt was unjustified…We found clear evidence of distortion of the truth…events such as the disappearance of records, although capable of innocent explanation, concerned us. We also found evidence of inappropriate distortion of the process of preparation for an inquest, with circulation of what we could only describe as ‘model answers’...Where individuals collude in concealing the truth of what has happened, however, their behaviour is inexcusable, as well as unprofessional.’ (p.8). ‘The Inquiry into Hyponatraemia-related Deaths’: This report by O’Hara was published in January 2018 following the investigation into the deaths of five children in Northern Ireland. ‘…concealment and deceit’ was identified. The Northern Ireland inquiry found that it was difficult to ‘…persuade some witnesses to be open and frank with the work of the Inquiry. All too often, concessions and admissions were extracted only with disproportionate time and effort. The reticence of some clinicians and healthcare professionals to concede error or identify the underperformance of colleagues was frustrating and depressing, most especially for the families of the dead children’ (p.25). There was a ‘…culture which concealed error’ (p.18), a failure to learn from the initial deaths and a great reluctance to admit fault. There was a ‘…underlying institutionalised reluctance to admit major shortcomings’ (p.111). ‘I am compelled to the view that clinicians did not admit to error for the obvious reasons of self-protection and that this defensiveness amounted to concealment and deceit’ (p.222) ‘…the unfortunate truth to be drawn from this Inquiry is that there are too many people in the Health Service who place reputation before honesty and avoidance of blame before duty’. (p.74). ‘The failure by senior clinicians to address the issue with appropriate candour suppressed the truth and inhibited proper examination of what had gone wrong.’ (p.98). Alison’s Story: This is a very tragic story. It is a very clear case of abuse of position and trust by a nurse. There is the inevitable ‘cover up’, and a catalogue of failures. There were people who should have taken action to protect Alison, but didn’t. Typical of many other situations in the NHS (e.g. deaths at Gosport hospital) some people did raise concerns, but nothing was done; classic NHS behaviour. Medical records were so-called ‘lost’ and the NHS organisation concerned did not share information with the police. ‘The truth was hidden to protect reputations’. lick here to edit. I recently watched “Panorama: Killed in hospital” (21 Jan 2019) detailing again the tragedy of 450 people having their lives shortened. At least another 200 people were probably similarly affected.
In 2018 the Gosport War Memorial Hospital report was published. It concluded that ‘…there was a disregard for human life and a culture of shortening the lives of a large number of patients by prescribing and administering “dangerous doses” of a hazardous combination of medication not clinically indicated or justified’ (Gosport Independent Panel, 2018, p.vii). The key phrase ‘make comfortable’ was identified in the Panorama programme as being repeatedly used in the medical notes. It was a rather sinister euphemism for hastening the death of a person. Many of the patients affected were actually sent to Gosport for rehabilitation. This situation goes to the heart of some of the aspects of severe dysfunction in the NHS. Evidence showed that nurses and relatives raised concerns over many years. The nurses were intimidated and ‘…felt ostracised’ (p.320). The warnings were ignored by managers, which resulted in the huge number of deaths between 1987 and 2000. People who raise concerns are often ignored across the NHS and in other so-called ‘care’ organisations. The Gosport situation again indicates that the NHS seems to be incapable of learning and improving. Another key dysfunctional cultural characteristic in the NHS is the lack of accountability. This was clearly identified in the Panorama programme. |

 RSS Feed
RSS Feed
